Indications
① Applicable situations
• Sensitive lesions near critical structures
Such as tumors close to major blood vessels, nerves, chest wall, or vital organs, where strict safety margins are required;
• Patients who cannot undergo surgery or are unsuitable for surgery
Including those with special tumor locations, multiple underlying conditions, or intolerance to general anesthesia, making surgical resection inappropriate;
• Patients with postoperative recurrence or strong local control needs
Can serve as part of local repeat treatment or a comprehensive therapy plan;
• Patients seeking minimal trauma and faster recovery
Especially suitable for elderly patients, those with multiple comorbidities, or those with high demands on quality of life.
② Common tumor types
• Solid tumors: liver cancer, kidney cancer, lung cancer, prostate cancer, bone tumors, etc., particularly for patients who cannot undergo surgery or need to preserve organ function.
• Benign lesions: breast fibroadenoma, uterine fibroids, etc.
Core Advantages
Cryoablation offers unique advantages for tumors located near critical structures or where traditional surgery carries high risks, especially for patients requiring both safety and functional preservation. Based on multidisciplinary assessment, this technique provides a gentle, controllable minimally invasive treatment option for complex lesions.
① Visualization with Low Temperature, Clear Safety Margins
During cryoablation, the formed "ice ball" is clearly visible under imaging, helping to judge the ablation range in real time and enhancing treatment control.
② Safer for Critical Structures
Low temperatures cause relatively mild damage to vessels, nerves, and other critical structures, reducing injury risk even without direct puncture.
③ Significant Analgesic Effect
The cold itself provides local anesthesia, resulting in relatively mild pain during and after the procedure.
④ Minimally Invasive, Fast Recovery
Treatment requires only a small percutaneous puncture, and most patients have a short recovery period.
⑤ Wide Indication Range
Applicable for multi-organ tumors, recurrent lesions, and elderly patients, providing treatment options for complex cases.
Why Choose Jinshazhou Hospital?
The hospital has performed over ten thousand cryoablation procedures, covering liver, lung, kidney, bone, head and facial regions, oral cavity, breast, prostate, and sarcomas, developing standardized processes and extensive experience in handling complex locations due to the high case volume.
The hospital is equipped with advanced cryoablation devices combined with CT and other imaging for precise localization, enabling visualized "ice ball" boundary control and enhancing treatment controllability and safety.
Procedures are performed by an experienced expert team, which, within the MDT framework, coordinates with radiotherapy and systemic therapy to design individualized plans; the hospital also continuously conducts clinical research and technical optimization in cryoablation, promoting iterative improvement and quality enhancement.
Technical Definition
Cryoablation is a minimally invasive treatment technique that destroys diseased tissue using extremely low temperatures. Argon and helium gases are delivered to the target area through a cryoprobe, causing the local tissue to undergo repeated cycles of rapid freezing and thawing in a short period, thereby inducing irreversible damage to tumor cells and rendering them nonviable.
This technique does not require open surgery and only needs local anesthesia, resulting in minimal trauma. It is an important component of the modern minimally invasive oncology treatment system.
Mechanism of Action / Working Principle
In an argon-helium cryoablation system, high-pressure argon gas rapidly cools the probe tip to approximately -140°C to -170°C, followed by rapid thawing using helium gas.
During repeated freeze-thaw cycles, intracellular water forms ice crystals that repeatedly melt, leading to disruption of the cell membrane and cellular structures. At the same time, local blood vessels undergo cryogenic occlusion, cutting off the tumor's blood supply and further exacerbating cellular damage.
After 2--3 freeze-thaw cycles, the tumor tissue gradually undergoes necrosis and is controlled. The entire process is conducted under imaging guidance to ensure precision and safety.
Treatment Procedure
① Preoperative Assessment: Evaluate the location, size, pathological type of the lesion, and the patient's overall condition.
② Imaging Guidance: Precisely locate the lesion using ultrasound, CT, or MRI.
③ Probe Placement: Insert the cryoprobe percutaneously or intraoperatively into the target area.
④ Freeze-Thaw Cycles: Rapidly cool to extremely low temperatures, maintain for several minutes, then allow natural thawing; typically repeated 2--3 times.
⑤ Probe Removal: Remove the probe after confirming the ablation area fully covers the lesion.
⑥ Postoperative Follow-up: Assess ablation effectiveness and monitor for recurrence through imaging review (e.g., contrast-enhanced CT/MRI).
Safety and Precautions
Cryoablation safety is based on precise control of the low-temperature effect range under imaging guidance. Prior to treatment, it is essential to carefully assess the spatial relationship between the tumor and nearby critical structures and to plan an appropriate puncture path. After the procedure, some patients may experience temporary local pain, swelling, or mild fever, most of which resolve spontaneously. Through standardized assessment and operation by an experienced team, the risk of complications can be effectively minimized.
Frequently Asked Questions
① How soon can normal activities be resumed after treatment?
Patients can generally resume daily activities within 1–2 weeks after the procedure, but it is recommended to avoid strenuous exercise and heavy physical labor.
② Is multiple treatment necessary?
Depending on the size and type of tumor, some patients may require multiple cryoablation sessions to achieve optimal results.
③ How long does it take to see the treatment effect?
Immediate effect: After cryoablation, patients usually notice reduced pain at the tumor site within a few days to a week, and the treated mass gradually decreases in size.
Final effect: Typically assessed 1–2 months later through imaging examinations (such as enhanced CT or MRI). Some patients may require further follow-up to ensure complete tumor ablation or to monitor for recurrence.
Typical Case
① Case 1:
Patient: Female, 17 years old, osteosarcoma
Presentation and Course: In the second half of 2024, the patient experienced a dragging and swelling sensation in the right lower limb. Further examination confirmed osteosarcoma. The lesion caused compression around the joint area, affecting walking. The patient and family explicitly refused surgical resection, emphasizing the desire to preserve limb function as much as possible and seeking a minimally invasive treatment with less trauma.
Treatment and Outcome: After admission, the patient underwent a multidisciplinary evaluation and received cryoablation. Post-treatment, the lesion volume decreased compared with before, symptoms were alleviated, and more favorable conditions were created for subsequent comprehensive treatment and further management.
Lesion Area
Ice Ball Formed by Cryoablation Probe During Treatment
Tumor Tissue Necrosis
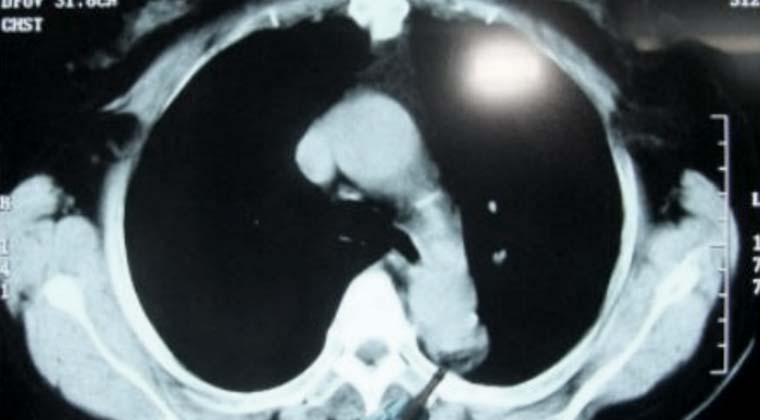
② Case 2:
Lesion in the left upper lung, adjacent to the aorta, considered a metastatic tumor.
Tumor Indicated by Probe Tip
Tumor Necrosis Area Indicated by Probe Tip
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501