Indications
① Applicable situations
• Locally controllable solid tumors: NanoKnife is a form of local therapy, typically used when tumor lesions are relatively confined, allowing targeted coverage with a clear treatment goal.
• Lesions adjacent to critical structures requiring both efficacy and structural protection: when tumors are near major vessels, gastrointestinal tract, bile ducts/gallbladder, pancreas, diaphragm, heart, or other key structures.
• Desire for local ablation while preserving critical structures: NanoKnife acts at the cellular level with minimal impact on fibrous and connective tissue, making it especially valuable in areas dense with important ducts, vessels, or nerves.
• Emphasis on individualized decision-making: for larger lesions or cases with distant metastases, the benefit of local ablation may be limited and should be evaluated by a specialist team to formulate an overall treatment strategy.
② Common indications
• Liver solid tumors, especially lesions close to the intestines or major vessels.
• Solid tumors in pancreas or other areas dense with vascular and ductal structures.
• Special sites in the liver, bile ducts, and pancreas region.
• Solid tumors in hilum areas of lung or kidney, where nerves and vessels are densely concentrated.
Core Advantages
• Non-thermal ablation mechanism: NanoKnife acts primarily through electroporation at the cellular level, rather than relying on heat or cold effects. For cases where traditional thermal or cryoablation struggles to balance \"safety margins\" with \"complete coverage,\" or where conventional surgery has limitations, NanoKnife provides a new treatment option.
• Emphasis on protecting critical structures: It has minimal impact on fibrous structures and connective tissue composed of proteins, offering a potential protective advantage for vessels, nerves, bile ducts, ureters, and other key structures within the target area.
• Suited for local treatment of high-risk tumor locations: Particularly advantageous for tumors near major vessels, gastrointestinal tract, biliary system, pancreas, heart, and other sensitive areas.
Why Choose Jinshazhou Hospital?
Our hospital introduced this cutting-edge minimally invasive technology in early 2022 and successfully performed NanoKnife ablation on two patients with malignant liver tumors. As one of the early adopters of this technology in Guangdong Province, we have accumulated valuable experience in standardizing new techniques, building procedural workflows, and clinical application.
NanoKnife treatment decisions at our hospital are carried out within a mature multidisciplinary (MDT) framework. For solid tumors such as those in the liver, the interventional/minimally invasive team leads the evaluation in collaboration with radiology, anesthesia, oncology, radiotherapy, and other relevant specialties: assessing whether the lesion is suitable for local therapy, evaluating the risk boundaries with major vessels, bile ducts, gastrointestinal structures, and determining if coordination with interventional, radiotherapy, or systemic treatment is necessary. After MDT discussion and formulation of an individualized plan, electrode placement and safety margin control are performed under image guidance, achieving a complete decision-making loop from eligibility assessment to treatment planning.
Within this MDT framework, NanoKnife is not just a single-point technique but a key tool within the hospital's comprehensive treatment system. It provides a new treatment option for complex cases that are not suitable for surgical resection or require high protection of critical structures, while also creating favorable conditions for subsequent combined therapy and ongoing management.
Technical Definition
NanoKnife (irreversible electroporation, IRE) is an innovative tumor ablation technology. By applying specific electrical pulses to the target area's cell membranes, it creates an irreversible electroporation effect, leading to tumor cell inactivation. Its characteristics are: the ablation primarily occurs at the cellular level without relying on extreme temperatures, causing no significant thermal changes; it is relatively more favorable for protecting critical tubular and scaffold-like structures within the target area, such as blood vessels, nerves, bile ducts, and ureters.
Mechanism of Action / Working Principle
Under imaging guidance, electrode probes are placed into or around the tumor target area. By delivering high-voltage electrical pulses, multiple nanoscale pores are formed on the tumor cell membranes, achieving an irreversible electroporation effect, thereby destroying tumor cells and inducing apoptosis.
Treatment Procedure
① Pre-procedure assessment: Complete imaging examinations to evaluate the lesion's location, extent, and relationship with critical structures, and develop an individualized treatment plan.
② Anesthesia and positioning preparation.
③ Image-guided percutaneous electrode placement: Under CT guidance, insert and arrange the electrodes according to the treatment plan.
④ Ablation procedure: Perform the planned electrical pulse ablation process.
⑤ Post-procedure evaluation: Assess the treated area using follow-up imaging.
⑥ Follow-up and reexamination: Conduct scheduled follow-up and monitor relevant indicators.
Typical Case
① Case 1:
Patient: Female, 70 years old, malignant solid liver tumor, lesion located near the intestine.
Procedure: Performed under general anesthesia. Using percutaneous puncture, two electrodes were placed to encompass the lesion, followed by ablation. During the procedure, the field strength remained stable, current increased significantly, and ablation was completed smoothly.
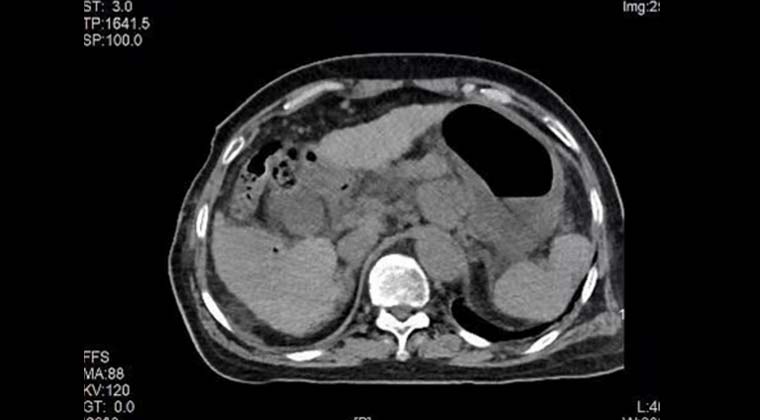
Post-procedure imaging: Enhanced CT showed clear lesion margins, with no significant enhancement in the ablation area.
Pre-procedure enhanced CT imaging
Pre-procedure electrode placement planning
Precise percutaneous puncture of the tumor under intraoperative CT guidance
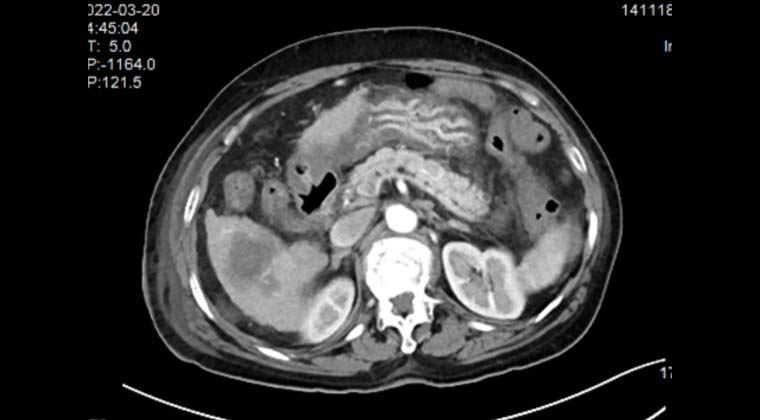
Immediate post-procedure non-contrast CT imaging
Enhanced CT imaging at 3-day post-procedure follow-up
② Case 2:
Patient: Male, 53 years old, malignant liver tumor
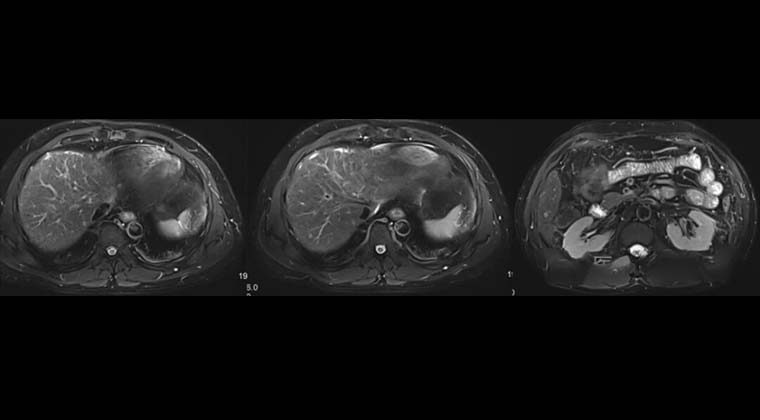
Preoperative MRI revealed three lesions adjacent to the intestine and blood vessels. Imaging findings: multiple nodular abnormal signal lesions in the liver, regular shape, unclear margins; T1WI iso-hypointense, T2WI slightly hyperintense; ADC values decreased; the largest lesion measured approximately 1.0 cm × 0.7 cm, showing marked enhancement in the arterial phase.
Diagnosis: Considering the unfavorable location of multiple lesions, close to the intestine and vessels, the risk of surgical resection was high with substantial trauma. Thermal ablation carried risks of incomplete ablation or vascular injury, making efficacy uncertain. NanoKnife ablation, with its non-thermal, selective ablation, was a better choice.
Preoperative CT localization was performed, and a precise needle ablation plan was formulated.
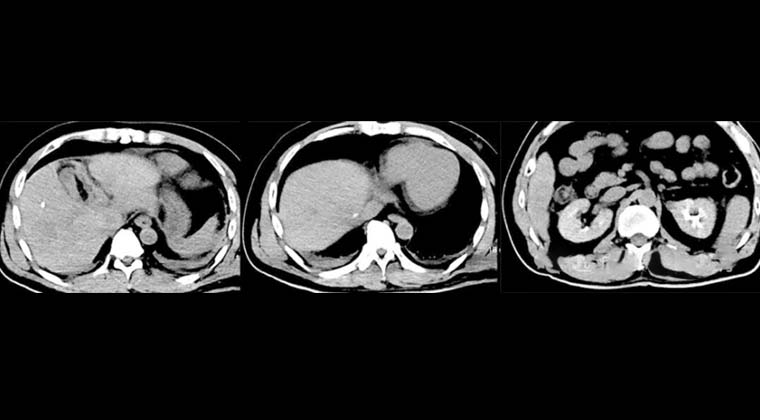
Immediate postoperative CT showed decreased lesion density, evident gas appearance, and intact surrounding critical structures such as vessels, indicating good and safe ablation results. After symptomatic supportive care, the patient recovered well.
Preoperative images
Immediate postoperative imaging
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501