TrueBeam High-Precision Image-Guided Linear Accelerator Radiotherapy
Applicable situations
① Typical scenarios better suited for TrueBeam
• Lesions with complex shapes or located close to critical organs.
• Tumors in the thorax or abdomen affected by respiratory motion.
• Multiple intracranial lesions requiring simultaneous treatment of several target areas.
② Common indications
• Head and neck: nasopharyngeal carcinoma, other head and neck tumors
• Thoracic: lung cancer, breast cancer
• Digestive system: esophageal cancer, gastric cancer, rectal cancer, primary liver cancer
• Gynecological: cervical cancer, endometrial cancer
• Genitourinary: prostate cancer
• Central nervous system: CNS tumors
Core Advantages
① Improved control over respiratory motion for more precise target coverage
TrueBeam is equipped with motion management features such as respiratory gating, allowing it to track breathing patterns. In thoracic and abdominal treatments where tumors move significantly with respiration, the system can deliver radiation at the optimal phase of the breathing cycle, ensuring better alignment with the tumor and minimizing unnecessary exposure to surrounding healthy tissue. In most cases, prolonged breath-holding is not required, making it easier for patients to cooperate and enhancing comfort.
② More efficient treatment, reducing discomfort from maintaining position
TrueBeam uses high-speed system control and stable beam output to support efficient delivery techniques like VMAT. This shortens the duration of individual treatment sessions, reducing the time and difficulty of maintaining position. The approach improves workflow efficiency while enhancing the patient experience.
③ Concentrated treatment for multiple intracranial lesions, saving time and streamlining workflow
With HyperArc technology, TrueBeam achieves sub-millimeter precision, enabling simultaneous irradiation of multiple tumors in a single session. The system automatically delivers each arc according to the planned sequence, without the need for manual couch adjustments during treatment. This workflow is efficient and safe, significantly improving treatment efficiency, especially for complex cases like multiple brain metastases that require high-precision, multi-target management.
④ Flexible selection of technical approaches by site and target, achieving better plan matching
The TrueBeam linear accelerator supports multiple radiotherapy techniques, including 3D conformal radiotherapy (3D-CRT), intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), image-guided radiotherapy (IGRT), and stereotactic body radiotherapy (SBRT). This allows clinicians to choose the most suitable approach based on the anatomical site and target characteristics, providing patients with a more personalized and comfortable treatment experience.
Why Choose Jinshazhou Hospital?
For international patients, the greatest challenge is often not the availability of technology, but whether treatment can be completed continuously according to plan within a limited stay. Our hospital is equipped with a comprehensive radiotherapy platform, including three TrueBeam linear accelerators, and has established flexible scheduling and patient flow management. This minimizes the impact of equipment maintenance and other factors on treatment schedules, reduces uncertain waiting and repeated trips, and helps overseas patients smoothly complete critical examinations, radiotherapy planning, and fractionated treatment, making the time cost of cross-border care more manageable.
Since the first HyperArc treatment in October 2020, our hospital has continuously developed related clinical practices and accumulated experience, gradually forming an implementation process for multi-target management, which provides mature procedural support for cases such as multiple intracranial targets. Additionally, our hospital integrates radiotherapy, imaging assessment platforms, and MDT multidisciplinary collaboration into a unified pathway, coordinating decision-making and treatment execution within the same framework. This improves cross-border communication and treatment continuity, allowing international patients to focus more on treatment and recovery itself.
To ensure the standardized implementation and continuous operation of this pathway, our hospital has established a full-process quality control system for radiotherapy. Quality control checkpoints are set from plan review and dose verification to treatment delivery, overseen by a team of radiotherapists, physicists, and technicians, ensuring consistency and traceability in plan execution. For international patients, this means a more controllable treatment process, clearer communication, and greater peace of mind.
Technical Definition
The TrueBeam system introduced at our hospital is a new-generation linear accelerator representing one of the most advanced designs worldwide, integrating multiple cutting-edge technologies. It can be used for a wide range of applications, including image-guided radiotherapy and radiosurgery. Equipped with the latest-generation HyperArc technology, its core strengths of high precision and high efficiency significantly enhance both the speed and accuracy of tumor treatment, enabling the system to meet the requirements of multiple radiotherapy techniques and diverse disease indications.
HyperArc is a non-coplanar stereotactic radiosurgery technology designed specifically for intracranial tumors, featuring a single isocenter with multiple targets. It is characterized by high precision, high efficiency, and a high level of automation. With sub-millimeter accuracy, it can complete stereotactic radiosurgical treatment of several to dozens of brain metastases within approximately 10 minutes, offering new therapeutic opportunities for patients with multiple brain metastases.
Mechanism of Action / Working Principle
① Biological effects of radiation
High-energy X-rays generated by TrueBeam penetrate the body and damage the genetic material of tumor cells, impairing their ability to grow and divide. Treatment is usually delivered in multiple fractions, allowing the tumor to be controlled through cumulative dose while providing normal tissues time to repair between sessions.
② Dose shaping and image localization
The system generates and delivers radiation according to the approved treatment plan. IMRT and VMAT achieve dose shaping through the coordinated use of a multileaf collimator (MLC), gantry rotation, and dose-rate modulation, allowing the dose to closely conform to the target while respecting organ-at-risk constraints. Before each session, two-dimensional and/or three-dimensional imaging is used for verification and, when necessary, positional correction (IGRT) to improve treatment consistency.
③ Respiratory motion gating
Using respiratory sensors or infrared cameras, the system tracks external markers on the patient's body surface to acquire real-time breathing signals. These signals are correlated with tumor motion to define a "respiratory window." Radiation is automatically delivered when breathing enters this window and the tumor position is closest to the planned target, and paused when it deviates, thereby reducing positioning uncertainty caused by respiratory motion.
④ HyperArc intracranial multi-target management
HyperArc employs a single-isocenter, non-coplanar VMAT stereotactic radiosurgery technique delivered on a linear accelerator. Its planning workflow is highly automated, enabling one-click arc generation, automatic optimization of collimator and gantry angles, and integration of tools such as SRS NTO (Normal Tissue Objective) and ALDO (Automatic Lower Dose Objective). This allows higher dose concentration within targets and rapid dose fall-off outside targets, improving plan reproducibility and delivery consistency in intracranial multi-target treatments and making the workflow more controllable.
Treatment Procedure
① Assessment and treatment planning
Based on disease stage, imaging findings, and overall physical condition, the suitability for radiotherapy is evaluated, and treatment goals and timing are defined. When necessary, the case is discussed within an MDT framework and coordinated with other treatment modalities.
② Immobilization and CT simulation
Patient immobilization is completed, followed by CT simulation in the treatment position (with respiratory-correlated scanning when indicated), providing the basis for treatment planning.
③ Target delineation and prescription
Target volumes and organs at risk are contoured, and the prescription dose and fractionation scheme are determined.
④ Plan design, review, and verification
IMRT, VMAT, or other appropriate treatment plans are generated, reviewed, and verified as needed to ensure clinical feasibility and safety.
⑤ Treatment delivery
A single treatment session is typically completed through the following four steps (time estimates are for reference only and may vary by treatment site and workflow):
• Precise positioning (approximately 5--8 minutes): Three-dimensional imaging is performed in the immobilized position for pre-treatment position verification.
• Intelligent alignment (approximately 1--2 minutes): Daily images are matched with the planned position, and corrections are applied when necessary using a six-degree-of-freedom treatment couch to improve positional accuracy.
• Precision irradiation (approximately 2--5 minutes): Dose is delivered according to the plan. With VMAT, the gantry rotates continuously, delivering modulated radiation from multiple angles while balancing efficiency and dose conformity.
• Rapid exit (approximately 1 minute): After irradiation, the patient can leave the treatment couch and room without the need for additional recovery procedures.
⑥ Recovery and follow-up
After completion of radiotherapy, physicians provide post-treatment guidance. Regular follow-up examinations are arranged to assess treatment efficacy and adverse effects, with adjustments or symptomatic management implemented as needed.
Frequently Asked Questions
① Does TrueBeam radiotherapy require special preparation?
Answer: Before treatment, disease evaluation, simulation positioning, and fabrication of immobilization devices (such as thermoplastic masks) are required. Patients need to cooperate with relevant examinations such as CT and MRI to determine tumor location and extent. During treatment, patients must maintain a stable position. Some patients may need to cooperate with respiratory gating technology and should undergo breathing control training in advance.
② How long does each treatment take, how many sessions are required, and is hospitalization necessary?
Answer: A single treatment session usually takes about 7--8 minutes. If special techniques such as respiratory gating are used, the duration may extend to 15--20 minutes. The total number of sessions and overall treatment course depend on tumor type, stage, and treatment plan. Most cases can be completed on an outpatient basis. Whether hospitalization is needed depends on the clinical condition and treatment plan. The medical team will evaluate and recommend the most appropriate care setting.
③ What should be done if discomfort occurs or travel plans change during treatment?
Answer: If discomfort occurs or schedule adjustments are needed, please inform the treatment team as early as possible. In most cases, continuity and safety of the treatment course can be maintained through reassessment and schedule adjustments.
④ What precautions should be taken during treatment?
Answer: Follow medical advice for skin care in the irradiated area. Keep the skin clean and dry. Avoid friction, hot or cold compresses, scratching, and the use of irritating products. Maintain a light and easily digestible diet, ensure adequate hydration, and adjust daily routines and activity levels as appropriate.
⑤ Can patients maintain a normal daily life during radiotherapy?
Answer: Patients can usually maintain a certain level of normal daily activities. It is recommended to keep close communication with the attending physician and adjust daily pace according to physical condition. If severe side effects occur, such as persistent fatigue, skin breakdown, or fever, patients should contact the medical team promptly and suspend normal activities, prioritizing health and recovery.
Typical Case
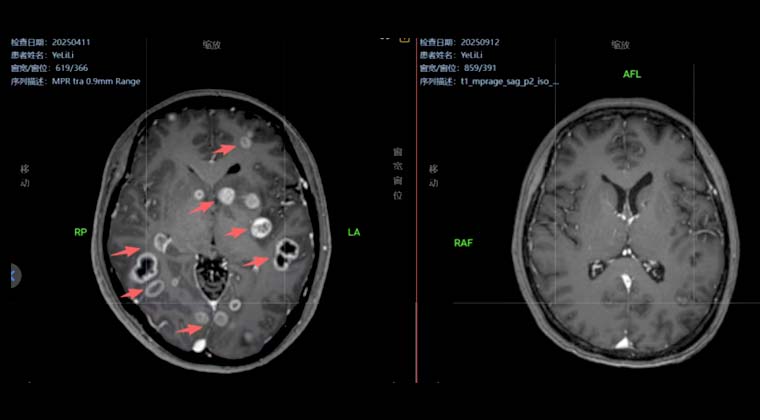
① Case 1:
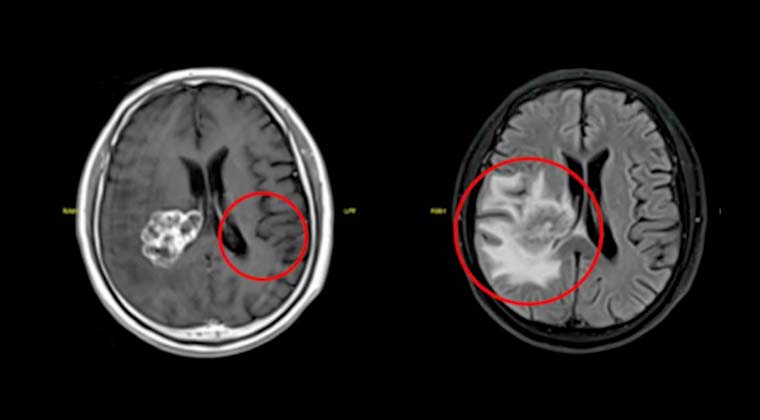
Female patient, 38 years old
History of comprehensive treatment for rectal cancer for nearly 3 years, with headaches for more than 1 month.
Diagnosis: Multiple brain metastases from rectal cancer (stage IVB, HER-2 positive). Previous chemotherapy and targeted therapy showed resistance, with multiple metastatic lesions in the brain.
In April 2025, SBRT (HyperArc stereotactic radiosurgery) was performed at our hospital for the intracranial lesions, 40 Gy / 10 fractions.
Five months after treatment, follow-up brain imaging showed near-complete regression of intracranial tumors (G-PR). The patient maintained a good quality of life.
Left image: Before treatment
Right image: After treatment
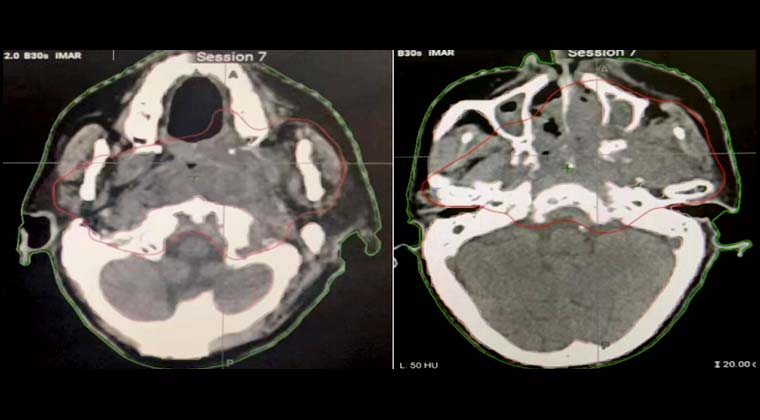
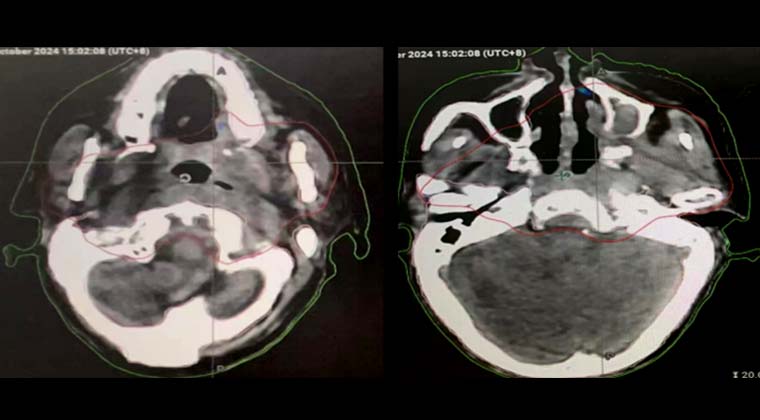
② Case 2:
Female patient, 76 years old
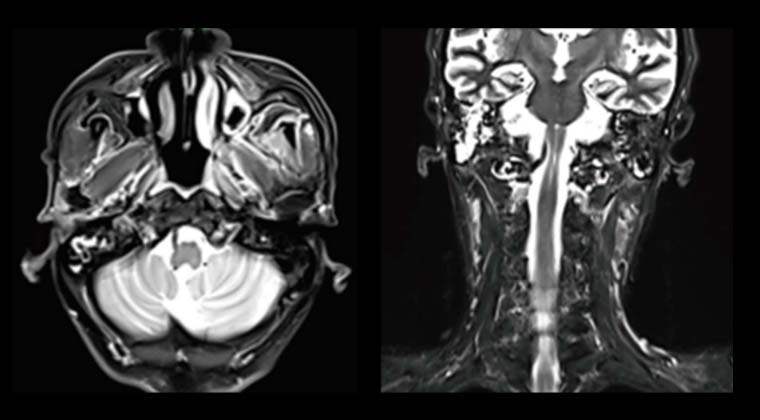
Diagnosed with nasopharyngeal carcinoma 5 years ago; did not receive standard chemoradiotherapy and managed the disease independently. One month ago, the patient experienced progressively worsening headaches, which became unbearable, accompanied by left eyelid drooping and hearing loss.
The patient and family requested symptom relief and pain reduction, refusing chemotherapy. Palliative radiotherapy was administered to the local tumor. The tumor was compressing the medulla oblongata, so a prescribed dose of 50 Gy / 25 fractions was set.
After 7 fractions of radiotherapy, the tumor showed significant shrinkage (red solid line indicates tumor range in the image), and the headache was relieved. The patient's confidence in treatment improved. The radiotherapy plan was then adjusted to include irradiation of the cervical lymphatic drainage area, and finally, the local tumor received a total curative dose of 70 Gy.
Before Treatment
After 7 fractions of radiotherapy
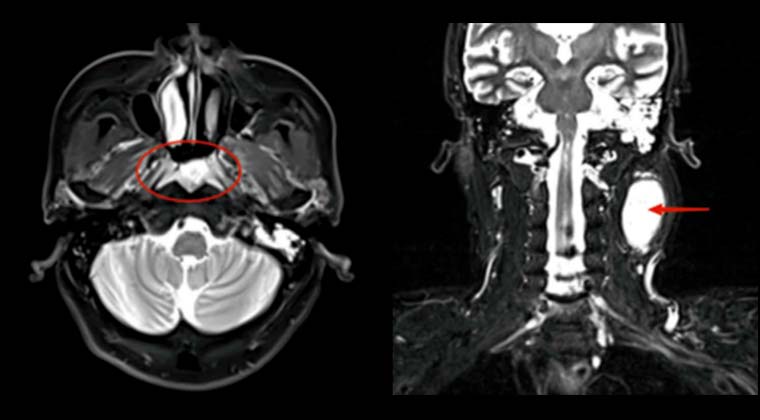
③ Case 3:
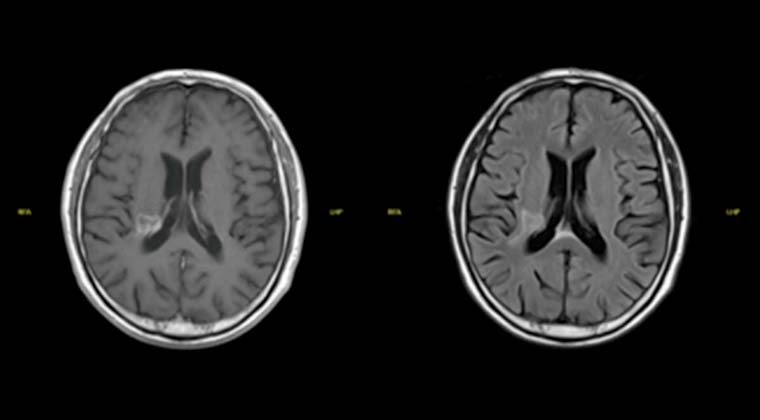
Patient: Male, 66 years old
Nasopharyngeal malignant tumor (nasopharyngeal undifferentiated non-keratinizing carcinoma)
From 2021‑04‑12 to 2021‑05‑27 underwent VMAT radiotherapy (PGTV 69.96 Gy / 2.12 Gy / 33 fractions)
Continuous follow-up after treatment showed gradual shrinkage of the nasopharyngeal lesion.
On 2023‑01‑05, MRI re-examination indicated the nasopharyngeal lesion had disappeared, and previously positive lymph nodes were significantly reduced.
Before Treatment:
After Treatment:
④ Case 4:
Patient: Male, elderly
Lung cancer with brain metastases, impaired brain function, uses a wheelchair
Before treatment: Severe peritumoral edema and high intracranial pressure
After treatment: Tumor regressed after 5 radiotherapy sessions
Post-treatment brain function recovered; the patient was able to walk independently
Before Treatment:
After Treatment:
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501