Stereotactic 3D radiotherapy (CyberKnife)
Indications
① Typical scenarios most suitable for CyberKnife
• Lesions that move significantly with respiration or organ motion (e.g., some lung, liver, or peri-pancreatic lesions).
• Lesions adjacent to critical structures requiring precise dose control (e.g., intracranial, paraspinal regions).
• Residual or recurrent lesions after previous treatment.
② Common indications
• Head and neck: primary tumors, re-irradiation.
• Lung: early and advanced primary lung cancer, lung metastases.
• Pancreas: patients unsuitable for surgery, preoperative or postoperative boost radiotherapy.
• Intracranial: brain metastases, primary tumors, trigeminal neuralgia, arteriovenous malformations.
• Liver: liver metastases, primary liver cancer unsuitable for surgery.
• Spine: spinal metastases, benign tumors, spinal arteriovenous malformations.
• Prostate: low- and intermediate-risk prostate cancer, monotherapy.
Technical Advantages
① Non-invasive, high-precision treatment: The CyberKnife uses omnidirectional central focusing and three-dimensional dose stacking, allowing the radiation to conform closely to the tumor's shape and position. With image-guided correction, it can achieve millimeter-level, and when necessary, submillimeter precision. Treatment does not require surgery or anesthesia, making the process more comfortable.
② Real-time image guidance and dynamic alignment: The system tracks the tumor dynamically using real-time imaging, ensuring each dose is delivered precisely to the target while minimizing exposure to surrounding healthy tissues.
③ Adaptation to tumor motion: For lesions that move with respiration (such as in parts of the lung, liver, or around the pancreas), the CyberKnife tracks the patient's position, tumor location, and respiratory motion in three dimensions and adjusts the beam direction in real time to match the tumor's actual position.
④ Precision near intracranial and spinal lesions: For tumors close to brain tissue, cranial nerves, or the spinal cord, treatment plans are designed with high precision to maximize protection of critical structures while adhering to strict dose constraints.
⑤ Concentrated treatment courses suitable for outpatient care: The CyberKnife is often used in regimens with a small number of sessions. Most patients can complete the treatment on an outpatient basis. The number of sessions is individualized based on tumor size, location, and tolerance of surrounding organs (commonly 1--5 sessions, with more in some cases).
Why Choose Jinshazhou Hospital?
Since 2019, our hospital has been using the CyberKnife M6 (the first in China) as a core device in the tumor radiotherapy center. The radiotherapy license was obtained in 2020, and the first treatment session using CyberKnife was completed on July 10, 2020.
Based on the CyberKnife M6 and other advanced radiotherapy platforms, we follow the principle of "individualized approach first": during MDT discussions, it is first assessed whether the patient is suitable for radiotherapy, the role and timing of radiotherapy in the overall treatment are determined, and coordination with surgery, interventional procedures, and systemic therapy is ensured. The radiotherapy team develops an individualized plan considering tumor location, proximity to critical structures, organ motion, and dose constraints, selecting the most appropriate platform and technical strategy rather than applying a "one-size-fits-all" approach.
The entire process is controlled through a closed-loop quality system: pre-treatment evaluation, plan verification, imaging-based corrections during therapy, and follow-up checks. This ensures that treatment is stable and manageable. Patients receive a comprehensive pathway: imaging evaluation, plan discussion, treatment planning, and therapy execution within the hospital, with integration with surgery, interventional, and systemic treatments when necessary. Key steps are under control, the treatment path is clear, and therapy is safe and reliable.
Technical Definition
The CyberKnife, also known as a "three-dimensional stereotactic radiosurgery robot," is a fully digital system with a conformal multi-leaf collimator for whole-body stereotactic X-ray radiosurgery. Our hospital has introduced the sixth-generation CyberKnife M6 by Accuray. It belongs to the category of stereotactic radiosurgery/radiotherapy (SRS/SBRT) and can track the patient's position, tumor location, and respiratory motion in three dimensions. During treatment, it adjusts the beam direction in real time under image guidance to precisely target the tumor or other treatment areas.
Mechanism of Action / Working Principle
① Omnidirectional Central Focusing and Three-Dimensional Dose Shaping
CyberKnife belongs to the category of stereotactic radiosurgery (SRS/SBRT). Its linear accelerator is mounted on a high-precision robotic arm, which can deliver fine beams from multiple angles around the patient. According to the treatment plan, these beams are superimposed within the tumor to create a three-dimensional dose distribution and precise shaping, concentrating the dose in the target while reducing exposure to surrounding healthy tissues. The radiation primarily damages tumor cell DNA, inhibiting replication and proliferation to achieve therapeutic effects.
② Image Guidance and Tracking Correction
CyberKnife uses imaging before and during treatment to verify and correct positioning. For lesions affected by respiratory or organ motion, strategies such as fiducial tracking or direct tumor tracking can be applied, allowing real-time adjustment of the beam according to tumor movement to ensure the radiation accurately matches the actual tumor position.
Treatment Procedure
① Assessment and preparation: The radiation oncologist evaluates the patient's condition, previous treatment history, and imaging to determine suitability for CyberKnife treatment and clarify treatment goals and timing; if necessary, an MDT discussion is held to coordinate with surgery, interventional therapy, or systemic treatment.
② Positioning and imaging acquisition: The patient is immobilized according to the treatment site, and a planning CT is performed (with MRI/enhanced CT or 4D-CT if needed) to obtain precise images for treatment planning. For lesions affected by organ motion, some patients may require implantation of fiducial markers (e.g., gold markers) under image guidance to support tracking strategies.
③ Target delineation and plan design: The radiation oncologist delineates the target and critical organs to protect; the medical physicist optimizes beam paths and dose distribution in the planning system and develops appropriate tracking/correction strategies; the plan is reviewed and approved by the team.
④ Treatment delivery: Before each session, image verification and positioning correction are performed; during treatment, the system monitors position using image guidance and applies necessary corrections/tracking, delivering multi-angle irradiation as planned. In most cases, anesthesia is not required, and treatment can be completed on an outpatient basis (subject to individual assessment).
⑤ Follow-up and review: After treatment, imaging and relevant tests are reviewed according to the follow-up schedule to assess efficacy and monitor reactions; any discomfort or worsening reaction should be promptly reported to the physician for management.
Frequently Asked Questions
① How many treatment sessions are needed with CyberKnife?
Answer: CyberKnife usually uses a small number of sessions, with many treatment plans completed in 1--5 sessions. The exact number is determined based on lesion size, location, respiratory influence, and tolerance of surrounding organs. The physician will create an individualized plan and explain the treatment schedule in advance.
② Does CyberKnife treatment cause pain?
Answer: CyberKnife treatment is completely non-invasive and involves no surgical incision, so it usually does not cause noticeable pain. The patient only needs to lie still on the treatment bed. Individual pain perception may vary, and in very rare cases, slight discomfort may occur due to tumor location or high sensitivity to pain.
③ Are there side effects from CyberKnife treatment?
Answer: Due to its high precision and non-invasive nature, CyberKnife has minimal side effects. Most patients experience no significant discomfort after treatment, though some may have mild skin reactions or temporary fatigue.
④ How soon can normal activities be resumed after treatment?
Answer: Most patients can resume daily activities on the same day or the next day after treatment. A few may experience temporary fatigue or minor discomfort, which typically resolves after a day or two of rest.
⑤ What precautions should be taken during and after treatment?
Answer: Skin care is essential during radiotherapy. Patients should follow medical guidance for cleansing, moisturizing, sun protection, and avoiding irritation. After the treatment course, follow-up should be performed as instructed, maintaining a regular schedule and moderate activity. Any significant discomfort or worsening reaction should be reported to a physician or nurse for assessment and management.
Typical Case
① Case 1:
Patient: Female, 10 years old
Diagnosis: Malignant brain tumor (glioma)
Symptoms: Weakness in legs and arms, unclear speech
CyberKnife treatment started on 2020-06-14, radiation dose PTV 25 Gy / 5 Gy / 5 fractions
At 2 months post-treatment, follow-up imaging showed slight reduction of the brainstem tumor. The patient regained consciousness, speech improved significantly, and limb movement gradually returned to normal.
Before Treatment:
After Treatment:
② Case 2:
Patient: Male, 67 years old
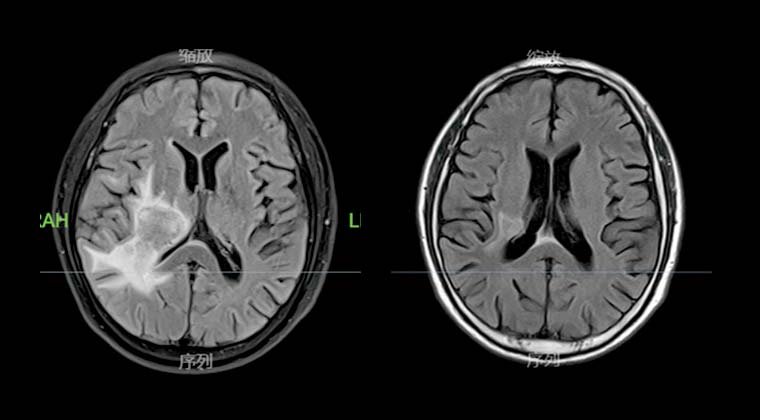
Secondary malignant brain tumor
Treatment with CyberKnife started on 2020-08-03, with a prescribed dose of 95% GTV DT15Gy delivered in 3 fractions of 5Gy each.
At 3 months post-treatment, imaging showed significant tumor reduction compared to previous scans.
Before Treatment:
After Treatment:
③ Case 3:
Patient: Female, 46 years old
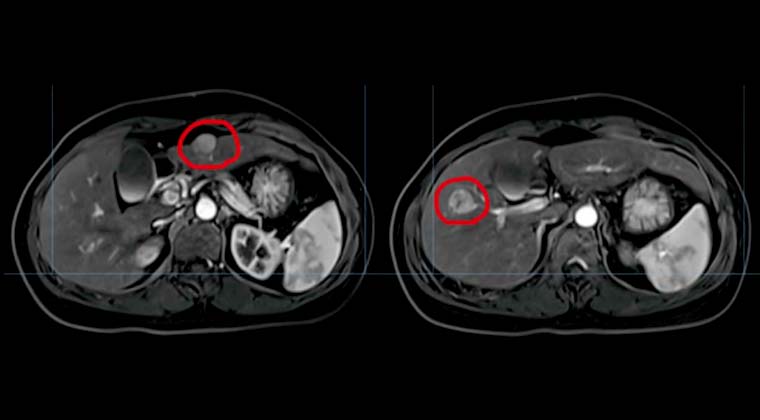
Diagnosis: Liver cancer
Treatment plan: 4D simulation and localization; lesions in segments S2 and S3 treated with DT 50 Gy / 10 Gy per fraction / 5 fractions.
Pre-treatment MRI at our hospital on 2020-12-06:
1. Multiple nodules in liver segments S2, S3, and S5; high possibility of small liver cancer.
2. Liver segment S6 hemangioma.
Follow-up MRI on 2021-04-14:
1. Post-comprehensive liver cancer treatment changes; lesions significantly smaller than before.
2. Gallbladder adenomyomatosis, largely unchanged.
Before Treatment:
After Treatment:
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501