Indications
① Primarily indicated for patients with malignant tumors in which the liver is the main site of disease:
• Primary liver cancer or liver metastases with predominantly intrahepatic lesions requiring enhanced local control;
• Patients who have lost the opportunity for surgery or are not suitable for radical resection, transplantation, or ablation (e.g., due to special tumor location or high surgical risk);
• Patients who may have surgical or transplant options but require "bridging therapy": for example, to control tumor progression and reduce tumor burden while awaiting liver transplantation;
• Patients with insufficient tumor control after other treatments, such as cases of colorectal cancer liver metastases that remain difficult to control after interventional or systemic therapy;
• Generally more suitable for patients with relatively preserved liver function and a tumor burden within an assessable range.
② Common tumor types
• Primary liver cancer
• Liver metastases: most commonly colorectal cancer liver metastases, and also liver metastases from other tumors such as neuroendocrine tumors and breast cancer
Key Advantages
① Combined "interventional + internal radiation" approach:
Microspheres are delivered via the arterial route into the tumor-feeding arteries. Unlike external irradiation, treatment is completed precisely within the liver, achieving localized internal therapy.
② Short β-particle range with limited radiation spread:
Yttrium-90 emits high-energy β radiation that mainly acts on tissues surrounding the microspheres. The limited penetration range helps increase the dose to the tumor target while minimizing exposure to surrounding normal liver tissue.
③ Sustained therapeutic effect after a single treatment:
Once deployed, the microspheres continuously release radiation over several weeks, providing a relatively stable local treatment period and facilitating subsequent comprehensive therapy planning and assessment.
④ Precise planning with individualized dose and delivery positioning:
Before treatment, tumors and their feeding vessels are systematically evaluated to define vascular anatomy, collateral branches, and perfusion territories. Based on this assessment, individualized dose calculation and delivery strategies are designed to improve precision and safety margin control.
⑤ Creating opportunities for subsequent treatment:
For some patients, the value of Y-90 therapy lies not only in completing a single procedure but also in creating conditions for further treatment. When intrahepatic tumor burden is the main limiting factor, Y-90 is often incorporated into MDT-based strategies in combination with immunotherapy, targeted therapy, or chemotherapy to strengthen local control and improve overall treatment feasibility.
Why choose Jinshazhou Hospital?
Since July 2023, when our hospital obtained qualification for yttrium-90 microsphere therapy, we have completed several hundred related procedures, establishing reproducible standardized workflows and stable clinical experience. This enables us to provide more targeted options for patients with malignant liver tumors characterized by large tumor burden, high surgical difficulty, unresectability, or poor control with other treatments.
Our advantages lie not only in the ability to perform the procedure, but in the level of refinement with which it is carried out. Relying on the platform of the International Precision Oncology Center, our hospital adopts multidisciplinary team (MDT) evaluation as the starting point, integrating interventional medicine, oncology, imaging, hepatology, and other key disciplines. From liver functional reserve and tumor burden to vascular anatomy, each aspect is systematically assessed to clarify risks and treatment pathways before implementation. During treatment, individualized dose calculation and delivery strategies are emphasized, with standardized procedures and strict quality control applied throughout preoperative planning, intraoperative execution, and postoperative follow-up, aiming to enhance local tumor control while protecting normal liver tissue and maintaining overall treatment tolerability.
Looking ahead, our hospital will continue to refine the standardized pathway of "precision assessment -- minimally invasive local therapy -- coordinated comprehensive treatment," leveraging more mature experience, closer multidisciplinary collaboration, and stricter process management to secure treatment opportunities and improve quality survival for more patients with complex liver tumors.
Technical definition
This is an advanced transarterial minimally invasive precision internal radiation therapy specifically targeting malignant liver tumors, combining embolization with internal radiotherapy. It is mainly used for primary liver cancer and various types of liver metastases.
Through femoral artery puncture, microspheres loaded with the radioactive isotope yttrium-90 are precisely delivered to the tumor site, where they continuously emit high-energy beta radiation. Beta radiation has a short penetration range and high precision, effectively destroying tumor cells and reducing tumor volume while sparing normal tissues. A single treatment can exert its therapeutic effect for several weeks.
Working principle / mechanism
Radioactive microspheres are precisely delivered to the tumor site via the femoral artery, where they release high-energy beta radiation. Beta radiation has a short penetration range and high precision, allowing targeted destruction of tumor cells while maximally preserving normal tissues. A single treatment can exert therapeutic effects for several weeks.
Treatment process
① Pre-treatment evaluation
Assessment of tumor distribution, hepatic functional reserve, and overall clinical status. When necessary, the treatment strategy is determined through MDT discussion.
② Vascular assessment and "simulation / rehearsal"
Angiography and related examinations are performed to identify tumor-feeding arteries, collateral branches, and perfusion territory, in order to select the most appropriate delivery position and access route.
③ Individualized dose planning
Dose planning is carried out based on evaluation data, with customization of the Yttrium-90 microsphere dose, balancing adequate tumor dose coverage and protection of normal liver tissue.
④ Interventional treatment implementation
Through femoral artery puncture and catheterization, the catheter is advanced under imaging guidance into the main tumor-feeding arterial branches, and Yttrium-90 microspheres are delivered according to the planned protocol.
⑤ Post-treatment observation and follow-up
Short-term observation is followed by scheduled imaging and liver function reassessment to evaluate microsphere distribution and local response, with coordination of subsequent comprehensive treatments when indicated.
Safety and precautions
Radioactivity decreases over time: the radioactivity of Yttrium-90 gradually decays with time. After treatment, follow-up examinations and daily life management should be carried out according to medical advice. In general, no special radiation shielding is required, but hospital-provided radiation safety guidance should still be followed.
Frequently asked questions
① Is multiple treatment required?
Yttrium-90 therapy is generally performed as a single treatment. The goal is to achieve adequate coverage of the tumor-supplying arterial territory with microspheres and allow them to exert a sustained local effect, so repeated procedures are usually not necessary. Whether repeat treatment or additional local or systemic therapy is required should be determined based on post-treatment imaging follow-up and MDT evaluation.
② What are the common adverse reactions?
Most adverse reactions are short-term and manageable. Common ones include fatigue, low-grade fever or fever (possibly related to tumor necrosis and absorption response), nausea, decreased appetite and other gastrointestinal discomforts, as well as upper abdominal or liver area discomfort/pain (which may be related to local inflammatory response, tumor necrosis, or liver tissue swelling with capsular irritation). If persistent high fever (≥38.5 °C), severe vomiting with inability to eat, pain that is difficult to relieve, or sudden worsening of symptoms occurs, timely medical attention is recommended.
③ How long does postoperative recovery take?
Most patients experience gradual relief of discomfort and can resume light daily activities within a few days after the procedure. It is generally recommended to avoid strenuous exercise and heavy physical labor for 1--2 weeks, and to undergo follow-up liver function tests and imaging as advised to assess treatment response. The specific recovery time depends on baseline liver function, tumor burden, and individual response, and should be guided by the attending physician's recommendations.
Typical case
Patient: male, middle-aged, hepatocellular carcinoma
Clinical presentation: The patient was diagnosed with advanced hepatocellular carcinoma during a routine physical examination, with a massive liver tumor and portal vein tumor thrombus. The disease progressed rapidly, with a marked decline in quality of life.
Treatment course: The patient presented to our hospital in February 2024. Prior to treatment, a Yttrium-90 simulation assessment was performed: MAA was injected into the tumor-feeding artery, followed by SPECT scanning to confirm blood flow distribution and safety margins. Subsequently, Yttrium-90 resin microsphere therapy was carried out, with the calculated dose of microspheres delivered as planned into the tumor-feeding arteries to achieve adequate lesion coverage.
Early postoperative period: In the early postoperative stage, the patient experienced mild fatigue, decreased appetite, and low-grade fever. These symptoms gradually resolved with symptomatic management.
Follow-up and outcome: Follow-up examinations demonstrated significant tumor shrinkage and regression of the portal vein tumor thrombus. Imaging findings indicated a necrotic response of the lesions. After MDT evaluation confirmed eligibility for surgical resection, further surgery was performed to remove the necrotic tumor. Pathological examination confirmed tumor necrosis. The patient's overall condition gradually improved, with a corresponding improvement in quality of life.
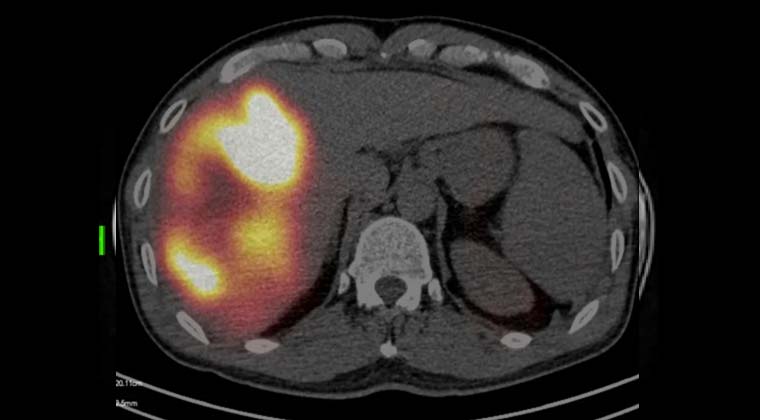
Imaging studies show a giant tumor with a diameter of 16 cm in the right lobe of the liver
Complete coverage of the giant tumor achieved with Yttrium-90 microspheres
Post--Yttrium-90 treatment imaging
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501