Indications
① Applicable situations
• Hypervascular tumors, large-volume tumors, or lesions that are difficult to achieve complete ablation in a single session
• Patients who are not candidates for surgery or have a high surgical risk
• Patients for whom improved conditions are needed to facilitate subsequent treatments
• Patients in whom reduction of recurrence risk or delay of disease progression is desired
② Common indications
• Primary liver cancer
• Liver metastases, such as colorectal cancer liver metastases
• Hypervascular tumors of organs such as the kidney and lung
• Other regionally confined solid tumors that are not suitable for surgical treatment
Core Advantages
① Minimally invasive with rapid recovery: Performed via limited transarterial puncture, resulting in minimal trauma, faster postoperative recovery, and reduced physical burden and hospitalization time.
② Precise targeting: Acts directly on tumor-feeding arteries, enhancing treatment efficacy and tumor growth control while maximally preserving normal tissues.
③ Low systemic side effects: As the treatment is localized to the tumor, drugs or embolic materials do not distribute widely systemically, leading to fewer systemic adverse effects and better patient tolerance.
④ Technical synergy: Interventional therapy can be combined with other modalities such as ablation, radiotherapy, and systemic therapies to strengthen the overall treatment strategy and improve outcomes.
⑤ Creates a window for subsequent treatment: Precise local control can effectively reduce tumor volume and slow progression, creating favorable conditions for follow-up therapies.
⑥ Multiple approaches with flexible strategies: TACI, TACE, and D-TACE can be individually selected based on tumor vascularity, extent, liver function reserve, and treatment objectives.
Why choose Jinshazhou Hospital?
Vascular interventional therapy is one of the most mature and clinically extensive core components of our hospital's minimally invasive oncology system. Our institution has outstanding technical expertise and rich clinical experience in the field of vascular intervention. Built on a large volume of accumulated clinical practice, the interventional team is led by senior department directors and principal operators, enabling more refined treatment planning tailored to the vascular characteristics of different tumors and individual patient differences. With advanced imaging navigation and DSA guidance, superselective catheterization of tumor-feeding arteries allows drugs and embolic materials to be delivered more precisely to the lesion, helping patients achieve solid local tumor control with minimal trauma.
We adhere to an MDT-based decision-making model as the starting point of treatment. Key issues---such as which modality to choose (TACI/TACE/D-TACE), treatment intensity per session, whether staged procedures are required, and whether to combine with ablation or systemic therapy---are fully discussed before the procedure. After treatment, efficacy and tolerance are continuously assessed through follow-up and imaging review, allowing timely optimization of subsequent strategies. Our goal is not merely to complete a single interventional procedure, but to help patients achieve more stable tumor control under manageable risk, while creating better conditions for subsequent comprehensive treatment.
Technical Definition
Minimally invasive interventional therapy (TACI/TACE/D-TACE) refers to a group of transarterial interventional treatments. Under imaging and DSA guidance, a catheter is selectively advanced into the tumor-feeding artery, delivering therapy "close to the lesion" to achieve local tumor control.
Among these, TACI is primarily based on transarterial infusion chemotherapy; TACE combines infusion chemotherapy with embolization; D-TACE (drug-eluting bead transarterial chemoembolization) involves loading chemotherapeutic agents onto microspheres, enabling embolization together with sustained local drug release.
Working Principle / Mechanism
① TACI: Local "infusion-based" drug delivery
Chemotherapeutic agents are infused via a catheter into the tumor-feeding artery, creating a higher local drug concentration within the lesion, thereby controlling tumor growth and reducing tumor volume.
② TACE: A "dual hit" of drug delivery plus embolization
After local drug administration, embolic materials are used to block the tumor blood supply, placing the tumor in an ischemic and hypoxic state. At the same time, the drug remains longer within the target area, enhancing local cytotoxic effects and tumor shrinkage.
③ D-TACE: "Sustained embolization plus slow drug release"
Chemotherapeutic agents are loaded onto embolic microspheres and delivered into the tumor vascular bed under DSA guidance. The microspheres both embolize the feeding vessels and gradually release the drug locally, achieving a more sustained combined effect of blood supply interruption and drug delivery, thereby strengthening long-term tumor control.
Treatment Procedure
① Preoperative Assessment: Imaging examinations plus liver/kidney function and coagulation evaluation; MDT discussion if necessary to determine the treatment plan and scope.
② DSA Angiography: Identify tumor-feeding arteries, communicating branches, and high-risk vessels.
③ Super-selective Catheterization: Access the main tumor-feeding branches whenever possible.
④ Treatment Implementation:
• TACI: Perform intra-arterial drug infusion according to the plan;
• TACE: Combine drug infusion with embolization;
• D-TACE: Deliver drug-loaded microspheres to achieve embolization and local sustained drug release.
⑤ Postoperative Observation and Follow-up: Monitor patient response and liver function changes; follow planned imaging follow-up to evaluate efficacy and decide the next steps.
Safety and Precautions
① MDT and Preoperative Assessment as Safety Prerequisites: Prior to treatment, systematically evaluate liver function reserve, tumor burden, vascular anatomy and communicating branches, coagulation status, and prior treatments within the MDT framework; select the most suitable TACI/TACE/D-TACE strategy and treatment scope accordingly.
② Strict Imaging Guidance and Precise Delivery: Perform the procedure entirely under DSA and other imaging guidance; emphasize super-selective catheterization of feeding arteries to reduce risk to normal liver tissue and non-target organs.
③ Common Postoperative Reactions and Observation Points: Some patients may experience fatigue, reduced appetite, mild fever, nausea, or discomfort in the liver area; these are usually short-term. Monitor temperature, pain level, food intake, and mental status as prescribed.
④ Situations Requiring Vigilance and Immediate Medical Attention: Persistent high fever, severe or progressive abdominal pain, repeated vomiting with inability to eat, worsening jaundice, bleeding tendencies, altered consciousness, or other unusual symptoms compared to previous conditions should prompt immediate contact with a physician or urgent care.
⑤ Puncture Site Care and Activity Management: Follow medical instructions for bed rest and lower limb immobilization; keep puncture sites clean and dry; avoid strenuous activity and heavy labor short-term. Report puncture site bleeding, enlarging hematoma, or limb numbness/pain promptly.
⑥ Liver Function Protection and Follow-up Assessment: Post-intervention, follow scheduled liver function tests and imaging to evaluate local control, determine whether staged re-intervention is needed, and assess readiness for subsequent ablation, radiotherapy, or systemic therapy.
⑦ Coordination of Combined Therapy by MDT: Interventional therapy is often combined with chemotherapy, targeted therapy, immunotherapy, radiotherapy, or ablation. The sequence, intervals, and medication regimens should be dynamically adjusted by MDT based on tolerance and efficacy; do not alter or interrupt follow-up independently.
Frequently Asked Questions
① Is hospitalization required for the procedure?
Most patients need to stay in the hospital for 1--2 days for observation; in some cases, a longer stay may be necessary.
② How soon can normal activities be resumed after treatment?
Generally, patients can resume daily activities within 1--2 weeks post-procedure, but strenuous exercise should be avoided.
③ Is multiple treatment required?
Interventional therapy is usually repeatable and can be staged. Depending on the patient's condition, some tumors may require multiple sessions to achieve optimal effect. The exact number depends on tumor response, liver function tolerance, and the plan for subsequent combined therapy; follow-up results and physician guidance should be used.
Typical Case
① Case 1:
Patient: Male, 41 years old
Hepatocellular carcinoma, BCLC stage C / CNLC IIIa
Symptom: Abdominal pain
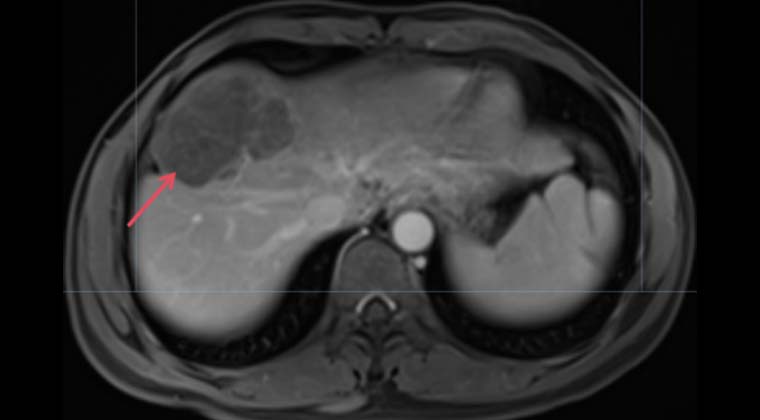
Diagnosis: 09-21 PET-CT showed a large lesion in the right liver lobe
Treatment Plan:
09-27: Abdominal aortic angiography, right renal artery angiography, superselective angiography + embolization of right diaphragmatic artery, celiac trunk angiography, superselective angiography + catheter placement in proper hepatic artery; intraoperative embolization with 1 ml iodized oil; postoperative arterial infusion of oxaliplatin 130 mg d1 + 5-FU 3.8 g over 46 h + leucovorin 300 mg d1; 09-29 arterial infusion of adebrelimab 1200 mg + intravenous targeted therapy with bevacizumab 810 mg (1 cycle).
10-18: Abdominal aortic angiography, right renal artery angiography, celiac trunk angiography, superselective angiography + catheter placement in right hepatic artery; postoperative arterial infusion of oxaliplatin 127 mg d1 + 5-FU 3.6 g over 46 h + leucovorin 300 mg d1; 10-21 arterial infusion of adebrelimab 1200 mg + intravenous bevacizumab 810 mg (2nd cycle).
11-16: Follow-up after two cycles of interventional infusion chemotherapy showed significant reduction of the lesion in the right liver lobe.
Pre-treatment Imaging
After-treatment Imaging
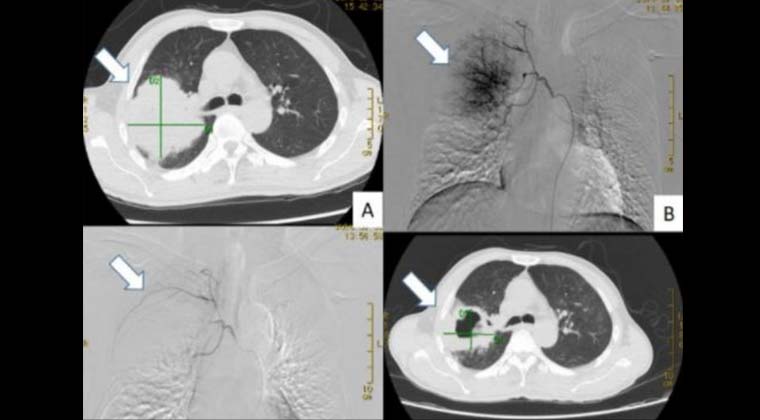
② Case 2: Bronchial Artery Chemoembolization
Patient with right upper lobe lung cancer, tumor diameter approximately 8 cm (top left image);
Drug-loaded microspheres were used for bronchial artery chemoembolization,
(top right image) imaging shows a clear tumor vascular network,
(bottom left image) post-embolization imaging shows complete disappearance of tumor staining;
One month after the procedure, follow-up imaging revealed significant tumor necrosis and shrinkage to about 4 cm (bottom right image).
The patient continued with comprehensive therapy, has survived for over a year, and remains under follow-up.
③ Case 3:
Patient, male, 75 years old, moderately differentiated transverse colon adenocarcinoma, with liver and bone metastases.
(Molecular testing: KRAS p.G12V mutation; BRAF V600E wild type; TMB 2.9; MSS; PD-L1 negative)
Chief Complaint and Clinical Course: Since May 2024, the patient experienced darkened stool (blackish-green well), followed by progressive fatigue. Previous hospital evaluation showed severe anemia (HGB ~40 g/L), imaging suggested a colonic mass with possible multiple metastases. Pathological biopsy confirmed moderately differentiated transverse colon adenocarcinoma. The patient was referred to our hospital for PET/CT evaluation, confirming transverse colon cancer with multiple liver and bone metastases.
Treatment Plan: Under DSA guidance, arterial interventional therapy was performed around tumor feeding arteries (super-selective angiography + tumor feeding artery embolization + arterial chemo-infusion), completed in four sessions on 07-26, 08-26, 10-16, and 11-06. The arterial infusion regimen included oxaliplatin (100 mg) combined with oral capecitabine (1 g, bid, d1--14) for palliative chemotherapy.
Treatment Response and Follow-up: Follow-up on 10-14 showed significant shrinkage of the primary transverse colon tumor; anemia improved markedly and the overall condition of the patient was enhanced.
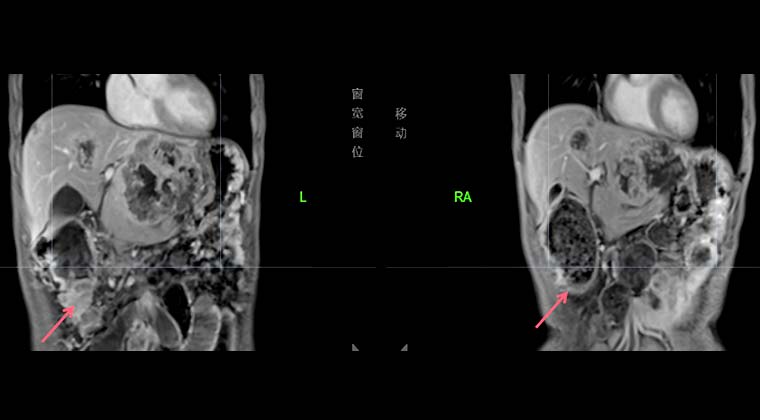
Left image: 2024-08-20, transverse colon tumor
Right image: 2024-10-14, transverse colon tumor significantly reduced compared with before, patient's anemia notably improved
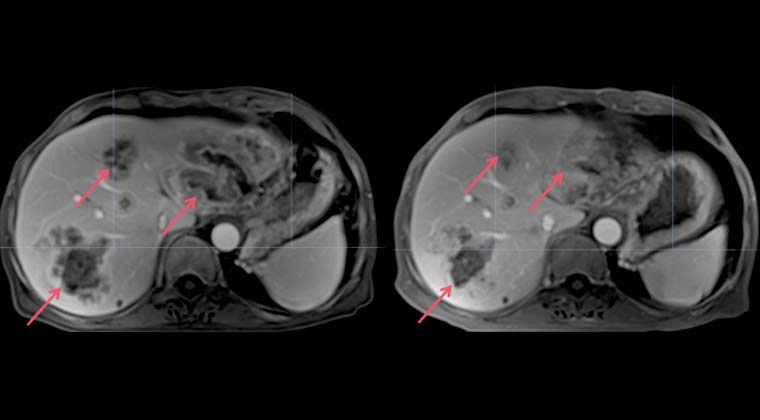
Left image: 2024-08-20, multiple liver lesions
Right image: 2024-10-14, liver tumors significantly reduced in size and number
 + 7 (700) 356-49-30
+ 7 (700) 356-49-30 Address
Address Email Form
Email Form Language
Language English
English

 + 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501
+ 7 (700) 356-49-30+ 86 13431079214+ 86 17688273501